New Guidelines for Postpartum Runners: Do not return to running until 12-week postpartum
Postpartum Mistakes
I made a lot of mistakes when I was returning to running postpartum in 2012. It was my second pregnancy, but my first postpartum experience as a “runner.” I’d just started to crack age group placings at local races and I was hungry to improve. I was so worried that I would lose all the hard work I’d put in over the last two years.
That fear, plus that fact that right around that time I joined Instagram and was suddenly bombarded with images of pregnant women running half marathons or marathons, made me feel like pregnant and postpartum runners just ran…a lot. Women wore running up until their due date as a badge of honor. It suddenly seemed like the norm and so naturally, I felt like if I was a runner that’s what I would do too.
Pushing too hard
So that’s what I did. I averaged 25-30 miles a week throughout my entire second pregnancy, ran a half marathon at 6 months pregnant and went running the day of my due date. For the most part I felt fine, but I leaked pee, had an occasional twinge here and there and was damn tired-maybe not directly after the run because those endorphins were flowing—but in general the fatigue got me. In retrospect, all that running on a lax pelvic floor was a HUGE NO-NO.

I had a natural childbirth with no complications on my end (our son however, did have a few complications) and immediately felt like I could take on the world. And so I did. Four weeks postpartum I was desperate for a run and went down to our basement treadmill. Everything felt fine until I picked up the pace a bit and suddenly I had this strong sensation that everything was “falling out” [you can read all about that experience HERE]. Turns out I had a mild bladder prolapse.

Will I ever run again?
Cue all the panic and fear of never being able to run again. Google wasn’t much help either. I couldn’t find anything about pelvic floor health except one woman who made a DVD you could order for $12.95, which I did. But otherwise there was nothing, just antiquated guidelines about heart rate and perceived exertion and nothing about pelvic floor health.
Thankfully I found a really great women’s health physical therapist locally [Cristin Zaimes at Oceanside Physical Therapy- who was recently on my Instagram Live Show] who helped me rehab my pelvic floor, reverse the prolapse and return to running. The next few years were some of my strongest ever as a runner.
New Study based on research and expert opinion
Running during and after my third pregnancy looked completely different, and every time I went in for an appointment with Dr. Zaimes we chatted about the lack of research around postpartum running. There still isn’t much in terms of clinical research studies, however official guidelines were recently (as of March 2019) released by a group of Physiotherapists from the United Kingdom, Tom Goom, Grainne Donnelly and Emma Brockwell.
Their study takes into account all the current research related to pelvic floor health and dysfunction and consolidates it into distinct guidelines for postpartum runners. While targeted towards health care professionals, it’s a document that anyone working with this population NEEDS to read and take into consideration.
Why? Because you shouldn’t be running until you are 12 weeks postpartum.
Wait until 12-weeks postpartum to begin running
Yup. Don’t @ me. That’s the new guideline and there is good evidence to support it. And to be clear, it doesn’t mean no activity it just means that running is ill-advised prior to 12 weeks. If you feel like you just could not possibly wait that long, don’t worry I’ve got some tips on what you can do in those 12 weeks for mental and physical health. But first, it’s critical to understand WHY waiting three months before resuming running is so important.
Why 3 Months?
Birth is beautiful. It’s painful. It’s difficult. Sometimes it goes how you imagined and other times it doesn’t. But no matter how you give birth: vaginally or by c-section, it is a trauma to the body. I don’t mean trauma in the sense of a traumatic emotional experience (although it can be that), I mean trauma to the soft tissues.
Think of all the expansion, stretching, sometimes tearing that goes on in a vaginal delivery. During the later stages of labor as the head descends into the birth canal the pelvic floor, specifically the opening in the pelvic floor called the levator hiatus must expand. One study showed that this expansion causes the muscles of the pelvic floor (the pubococcygeus, the iliococcygeus, and the puborectalis also known as the levator ani) to stretch up to 259% of it’s resting tone (Ashton-Miller et al. 2009). In the past, a guideline of 6-8 weeks was given to women for returning to run after pregnancy, but recent studies and general consensus is that the soft tissues are just finishing the healing process at that point and are still far from prenatal strength.
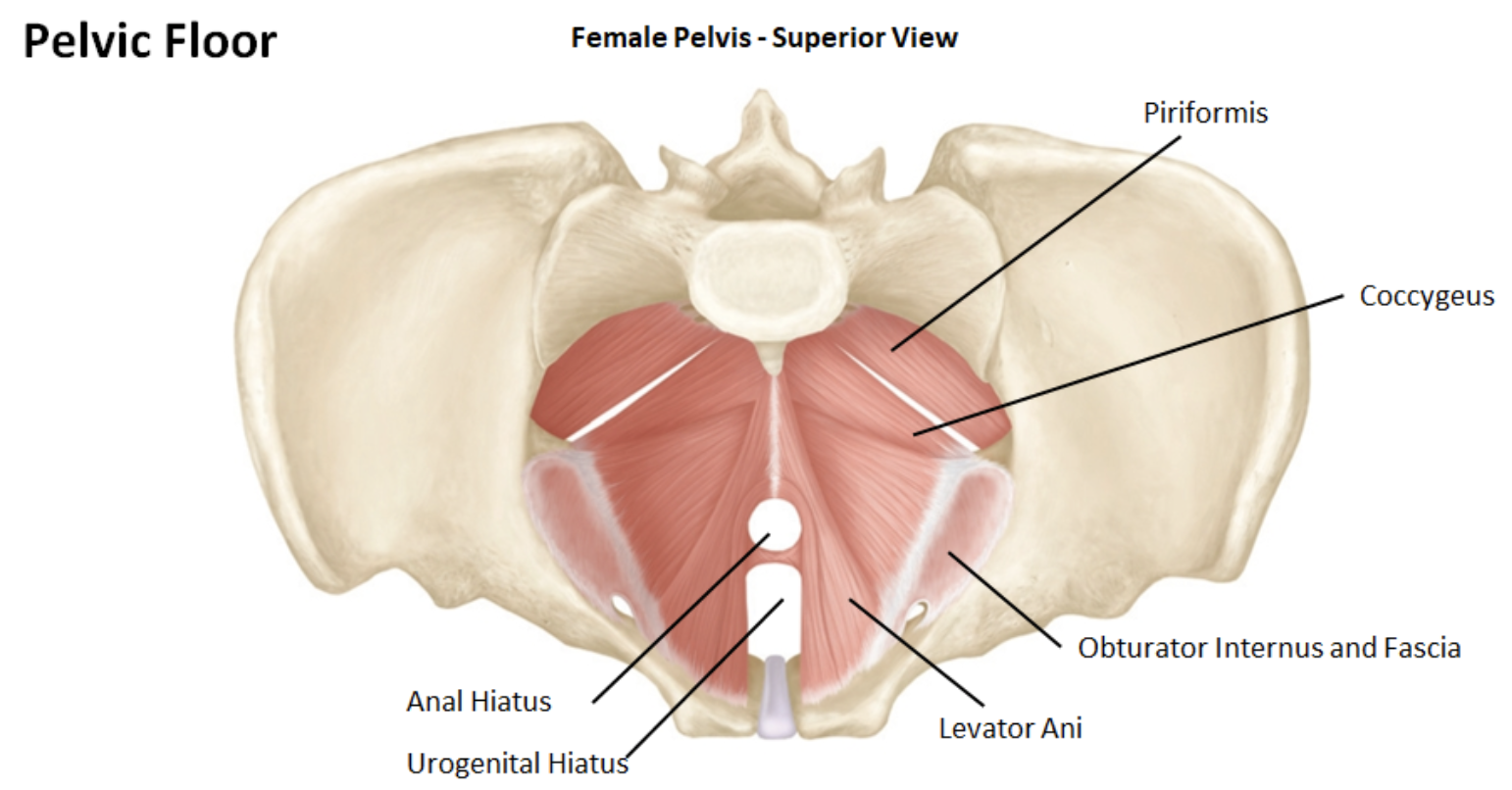
Image source.
A c-section is major abdominal surgery, cutting through skin, muscle, fascia and the uterine wall. Studies show that the uterine scar is still thickening (healing) at 6-weeks postpartum and that the abdominal fascia does not gain its original tensile strength until 6-7 months postpartum. Meaning that the previously accepted period of time for healing from a c-section may in fact be longer.
The Pelvic Floor
And if you haven’t done any pelvic floor strengthening prior to birth you are more likely to experience adverse symptoms during labor and delivery. Based on my personal experience, there was not a lot of education surrounding optimal pelvic floor health after labor and delivery, let alone going into it. I walked into birth blindly, with a little bit of information from our birth classes at the local hospital, but not much else. What I now know is that it’s just as important to be able to control the contraction of the pelvic floor as it is to be able to relax the pelvic floor. Control of those muscles greatly impacts the birth experience. It’s critical to be aware of your pelvic floor health leading up to labor and delivery so that the muscles are at optimal strength prior to birth. It also makes engaging the pelvic floor and conducting strengthening exercises postpartum much easier, since you already have experience. During my third pregnancy I had three prenatal appointments with my women’s health physical therapist to make sure pelvic floor strength was optimized and then work on techniques for relaxing the pelvic floor during delivery.

What does that mean for me?
Even if everything goes swimmingly at birth and you smooth delivery with no tearing, the muscles and fascia of your pelvic floor have done some considerable work and they are not ready for a high impact activity like running. It’s like the equivalent of whiplash, just inside and the stretching of all the soft tissue, instead of being instantaneous is prolonged-for however long that head is in the birth canal. Yet so many women are out there running long before their bodies have recovered. It’s possible that these women are asymptomatic, but unlikely since 11% of all women in the US undergo surgery for pelvic floor dysfunction(Ashton-Miller et al. 2009). If 11% require surgery, what is the continuum of women not needing surgery but still experiencing dysfunction? What’s more likely is that women are ignoring the warning signs and chalking it up to “I just had a baby and this is normal.”

Walking is a great low-impact activity for return to running postpartum.
Warning Signs
It is not normal to leak pee while running (or sneezing or coughing or jumping).
It is not normal to have pain during intercourse.
It is not normal to feel pressure or bulging in the pelvic area.
It is not normal to have low back pain or lumbo pelvic pain.
In fact, these are all symptoms of pelvic floor dysfunction and if you experience them you need to know what to do.
So what do you do? You find a women’s health physical therapist who specializes in pelvic floor health and schedule an appointment. That appointment will most likely include an internal exam (called the Modified Oxford Manual Muscle Test) where your PT will assess pelvic floor strength and function. During that exam they are testing for strength, speed of the contraction, coordination and function. For those scoring less than a grade 3 on this test or unable to meet a baseline test of pelvic floor endurance while standing, it is inadvisable to return to running until the pelvic floor has been strengthened further.
For many women this test shows one side is weaker than the other and that left-right asymmetry can cause problems on a grander scale: think running injuries down the line associated with asymmetrical weakness in the hips, like piriformis syndrome, high hamstring tendinopathy, IT Band syndrome and more. Regaining strength in the pelvic floor is critical for reducing future risk of injury.
If your PT finds weakness and dysfunction they will prescribe a series of exercises to strengthen the pelvic floor (usually kegel contractions at varying speeds and durations) and exercises to strengthen the abdominal wall (like abdominal bracing, bent knee drops, side lying leg raises, etc). Restoring optimal pelvic floor function is the goal and often requires at least three months of targeted strengthening before a maintenance routine can be adopted.
The baseline for pelvic floor strength and endurance recommended by Goom, Donnelly and Brockwell is:
10x fast contractions of the pelvic floor while standing (kegel)
8-12 reps of 6-8 second hold maximum voluntary contraction of the pelvic floor
60 second submaximal 30-50% contraction of the pelvic floor
What if I can’t find a PT?
If you are unable to find a PT in your area there are more subjective criteria you can use to assess readiness. If you answer ‘yes’ to any of the following criteria, then you should not return to running:
Leak pee at the start or at any point during a run
Feel pressure/bulging/dragging in the vagina at the start of running
Onset or ongoing vaginal bleeding (unrelated to your period) before or after low or high impact activity
Musculoskeletal pain before, during or after running including pelvic pain and lumbar pain
If these are your symptoms, avoiding running and focusing on pelvic floor rehabilitation should be the priority along with seeking a more formal assessment from a pelvic floor physical therapist. To strengthen the pelvic floor begin with the baseline pelvic floor contractions listed above. If the exercises cannot be performed while standing, modifying to a supine position with bent knees and then a seated position prior to progression to standing.
Important Considerations
The guidelines acknowledge that for so many women, running is a coping mechanism for mental health and I would not exclude myself from that category. However, they mention Postpartum Depression (PPD) as a risk factor for pelvic floor dysfunction because relying on running as a coping mechanism may in fact lead women to increase intensity and duration prior to healing of the pelvic floor. In this instance, finding alternative coping strategies are advisable and can include physical activity, like walking and hiking, but should include mental health counseling with a licensed therapist.
In addition, Relative Energy Deficiency in Sport (RED-S, formerly known as Female Athlete Triad Syndrome) is another indicator of risk related to pelvic floor dysfunction caused by postpartum running. If RED-S has been clinically diagnosed prior to or during pregnancy it is critical that postpartum return to running is monitored by a team of health professionals.
While the guidelines don’t directly cover Diastasis Recti (DR) it does mention that inconclusive and limited research has yet to show a direct correlation between pelvic floor dysfunction and DR. However, running with DR can cause overloading and compensation in the pelvic floor due to a weakened abdominal wall. Any presence of DR should be addressed with a physical therapist and optimal function should be achieved prior to return to running.
Running During Pregnancy
Though not mentioned in the study, prenatal anxiety and the previous diagnosis of RED-S prior to or during pregnancy could potential predispose women to pelvic floor dysfunction risk, for similar reasons related to intensity and duration, as they run throughout pregnancy. While individuals are different, it is important for women running through pregnancy to be aware of the importance of pelvic floor strength. In my opinion, a more conservative approach to running during pregnancy can lead to a quicker and less complicated return to running postpartum.
It is important to acknowledge the influence of social media as it pertains to running during pregnancy and postpartum, as social pressure and comparison can often influence how women approach running during this time. Which is why official guidelines are so necessary for clinical health professionals as well as non-clinical professionals who work with women during pregnancy and postpartum, including personal trainers, running coaches and fitness instructors.
So what the heck do I do for 12-weeks?
I’m so glad you asked! There is SO much that you can do for 12-weeks that doesn’t involve running, but can take its place temporarily so that when you do return you are stronger than ever.

Sleep: In the first few weeks after labor and delivery sleep should be your priority. Sleep is essential to recovery and healing. While this is the biggest priority it is also the most frustrating advice a women who just had a baby can possibly receive. When you have a newborn sleep is hard to come by. Napping while they nap doesn’t often work especially if there are older children in the household. If it is available, asking friends of family to come over during the day to let you sleep can be a huge help. But if that is not a realistic suggestion, when given the choice between folding the laundry, doing the dishes or your pelvic floor exercises, the best bet early on is to choose sleep.
Diaphragmatic Breathing: simple diaphragmatic breathing can be helpful as you work to strengthen the pelvic floor. A diaphragmatic breath involves contracting and relaxing the diaphragm. As you inhale the belly expands and pelvic floor relaxes. As you exhale the pelvic floor contracts upward as does the diaphragm, forcing the breath out. Practice 1 x 30 breaths daily.
Pelvic Floor Contractions: Daily pelvic floor exercises can begin immediately. Start in a supine position with knees bent or a seated position. Be sure the pelvis is in a neutral position. Perform the baseline exercises suggested by Goom, Donnelly and Brockwell
10x fast contractions of the pelvic floor while standing (kegel)
8-12 reps of 6-8 second hold maximum voluntary contraction of the pelvic floor
60 second submaximal 30-50% contraction of the pelvic floor

Walking or Treadmill Hiking: low-impact exercise during the first 12-weeks is a great way to build strength, get outside and take advantage of the mental health benefits of moving your body. Gently walking can be resumed whenever ready. Progress walking in distance prior to intensity. More vigorous walking or uphill walking on a treadmill can be introduce 4 to 6-weeks postpartum.
Basic Core Strength: basic core strength can begin with abdominal bracing lying on the floor then progress to a foam roller, working on pelvic floor engagement and “knitting the ribs together,” progress to bent knee drops. Bridges and side lying leg raises are great additional core exercises for the first few weeks postpartum.
Total Body Strength: around the 2 to 4-week mark, begin introducing gently body weight strength training. This can include squats, deadlifts, and lunges. As healing progresses, compound movements and light weights can be added around the 6-8 week mark, for example a squat with an overhead press.
When I do get back to running, what should I do?
When I returned to running after my third pregnancy, I took everything I had learned the hard way, plus new insights and recommendations from my PT and created an 8-week progressive running plan for myself that was low impact, yet built cardiovascular strength. I built a solid foundation and for the last five years have been able to run injury-free. That eight week program allowed me to ease into running postpartum with a combination of walking, hiking and uphill running. When I did resume regular training I was stronger and faster than I had been my two previous postpartum experiences.

A note to running coaches
If you work with runners who are returning to running postpartum it is important to be well-informed regarding pelvic floor dysfunction and optimal strength. These guidelines are incredibly important and in my opinion, should be adhered to unless an individual has been assessed by a women’s health physical therapist and cleared to return to running prior to 12-weeks postpartum. In the guidelines Goom, Donnelly and Brockwell outline a strength, load and impact assessment for postpartum runners. This assessment allows non-clinical professionals working with this population another tool for assessing running readiness. You can find that HERE.
-Sarah
Want to check out my training and daily musings? Follow me on Instagram.
Or connect with me here, I love getting emails from readers!
Email: sarah [at] sarahcanney [dot] com
Twitter: @sarahcanney
Facebook: Facebook.com/sarahecanney
Pinterest: pinterest.com/runfargirl